Avascular necrosis (AVN) of the femoral head is an increasingly common cause of musculoskeletal disability, and it poses a major diagnostic and therapeutic challenge. Although patients are initially asymptomatic, avascular necrosis (AVN) of the femoral head usually progresses to joint destruction, requiring total hip replacement (THR), usually before the fifth decade. In fact, 50% of patients with avascular necrosis experience severe joint destruction as a result of deterioration and undergo a major surgical procedure for treatment within 3 years of diagnosis. Femoral head collapse usually occurs within 2 years after development of hip pain. 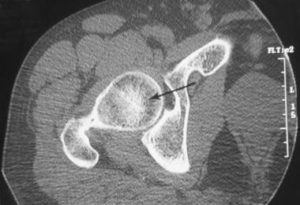
Axial computed tomography scan in a patient without avascular necrosis of the femoral head shows prominent and thickened but normal trabeculae (arrow) within the femoral head. Note the delicate, sclerotic, raylike branchings emanating in a radial fashion from the central dense band. This is the asterisk sign. See also the next image.
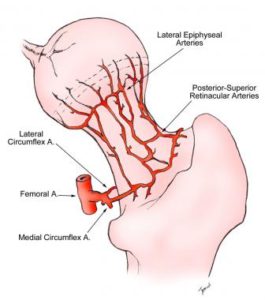
Avascular necrosis of the femoral head. Illustration of the normal circulation of the femoral head, viewed from the posterior approach. The posterior-superior retinacular arteries provide the major blood supply to the epiphysis. They traverse the femoral neck and are contained within the joint capsule and give rise to the lateral epiphyseal vessels at the junction of the femoral head and neck. From there, they penetrate the femur and supply the femoral epiphysis. A. = artery.
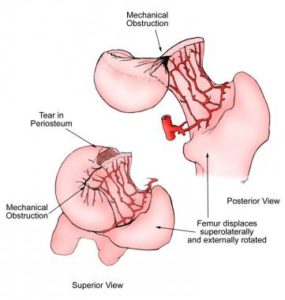
Avascular necrosis of the femoral head. Illustration demonstrating that the blood supply to the femoral head is compromised by subcapital femoral fractures or slipped capital femoral epiphysis. As the epiphysis or femoral neck separates from the femoral head, the femoral metaphysis displaces superolaterally and the femur rotates externally. This causes the distal posterior-superior retinacular arteries and proximal lateral epiphyseal vessels to kink or rotate, compromising the blood flow to the epiphysis. If this condition were to persist, the femoral head would be at high risk for developing avascular necrosis.

Frogleg lateral view of the right hip in a patient with avascular necrosis shows the crescent sign, indicating subchondral fracture. Therapeutic interventions are less likely to halt progression of the disease once this sign appears. The frogleg lateral view is better than anteroposterior (AP) projection for demonstrating this sign, because the anterior and posterior margins of the acetabulum on the AP projection are superimposed over the superior portion of the femoral head, the usual location of the sign.